Research
Studying outcomes in hip surgery using national datasets: What lessons can be drawn from analysing linked national datasets on revision hip replacement procedures?
Improved planning, smarter resource allocation and above all, better patient outcomes, are the aims of this research study, which is analysing revision hip replacement procedures handled by individual consultants across the country. Previous studies have focussed on the impact of the volume of procedures handled by specialist centres, but the researchers believe that it is only by also considering consultant level data that we can gain a true picture of what is happening.
Revision hip replacement, which involves a partial or a complete exchange of the prosthesis that was implanted during the original (‘primary’) surgery, is a complex procure and success rates vary widely. In this research project, funded by ORUK in partnership with the British Hip Society, the researchers analysed data from the National Joint Registry from 2011-2020.
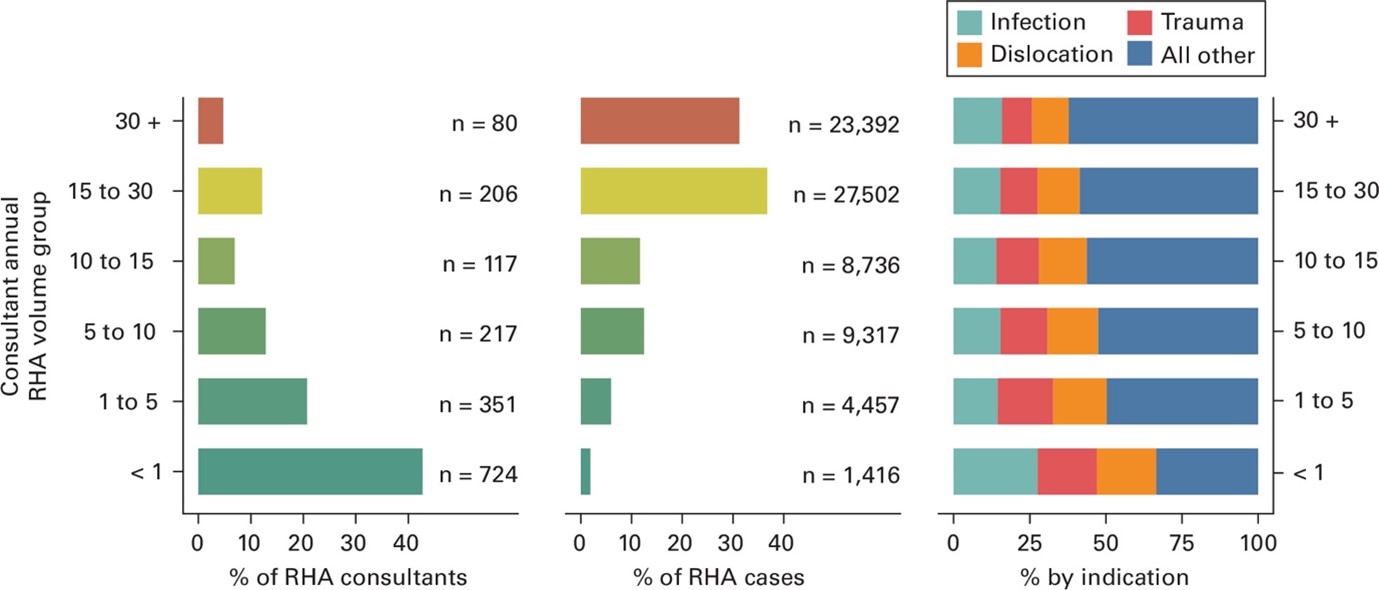
In their recently published article, the researchers were able to track the activity of individual consultants over almost a decade’s worth of data, including following a group of newly appointed surgeons. Their analysis shows that a relatively small number of highly experienced consultants are handling the majority of revisions, which is hardly surprising given the complexity of the procedure – around 75% of the revisions are done by the 20% highest volume surgeons (Figure). At the same time, there was considerable variation between the volumes that individual consultants are undertaking across the country – the vast majority of consultants are only handling a small number of revision procedures in a typical year, often less than one a year.
Furthermore, considering newly appointed hip surgeons collectively, their rate of gaining revision expertise was extremely low and the small minority who eventually undertook more than 15 such procedures annually may take more than five years to do so. Consequently, a key theme arising from the work is the importance of continuing education. Revision hip surgery is complex and requires sub-specialist training prior to becoming a consultant.
The group discovered that revision surgery performed for urgent problems, such as infection or where the bone around the hip replacement breaks, were more commonly performed by surgeons with less experience around weekends and bank holidays. Holleyman says, ‘It may be that less experienced consultants on call during the weekends are obligated on clinical grounds to undertake emergency procedures, for example where the patient is experiencing a life-threatening infection, even when such an operation may be outside their own area of expertise. In some situations, these less experienced consultants may, on average, have undertaken 40% fewer procedures in the previous year than their more experienced colleagues. This ‘weekend effect’ almost completely disappears when we looked at non urgent indications,’ in such cases where the patient can reasonably wait to be treated by the most appropriate surgeon.
This work emphasises the importance of building a wider pool of suitably experienced consultants such that patients can be treated by the most appropriate individual, whenever that care may be needed. Further work will continue to examine these associations.
Tell us your thoughts